
 Lost Souls Lost Souls
|
 Peds Atlas Peds Atlas
|
 Volumes Volumes
|
 Aortic Diameter - Adult Aortic Diameter - Adult
|
 Kidney Size - Peds Kidney Size - Peds
|
 Spleen Size - Peds Spleen Size - Peds
|
 Testicular Volume Testicular Volume
|
 Lung Nodule 2017 Lung Nodule 2017
|
 Contact Contact
|
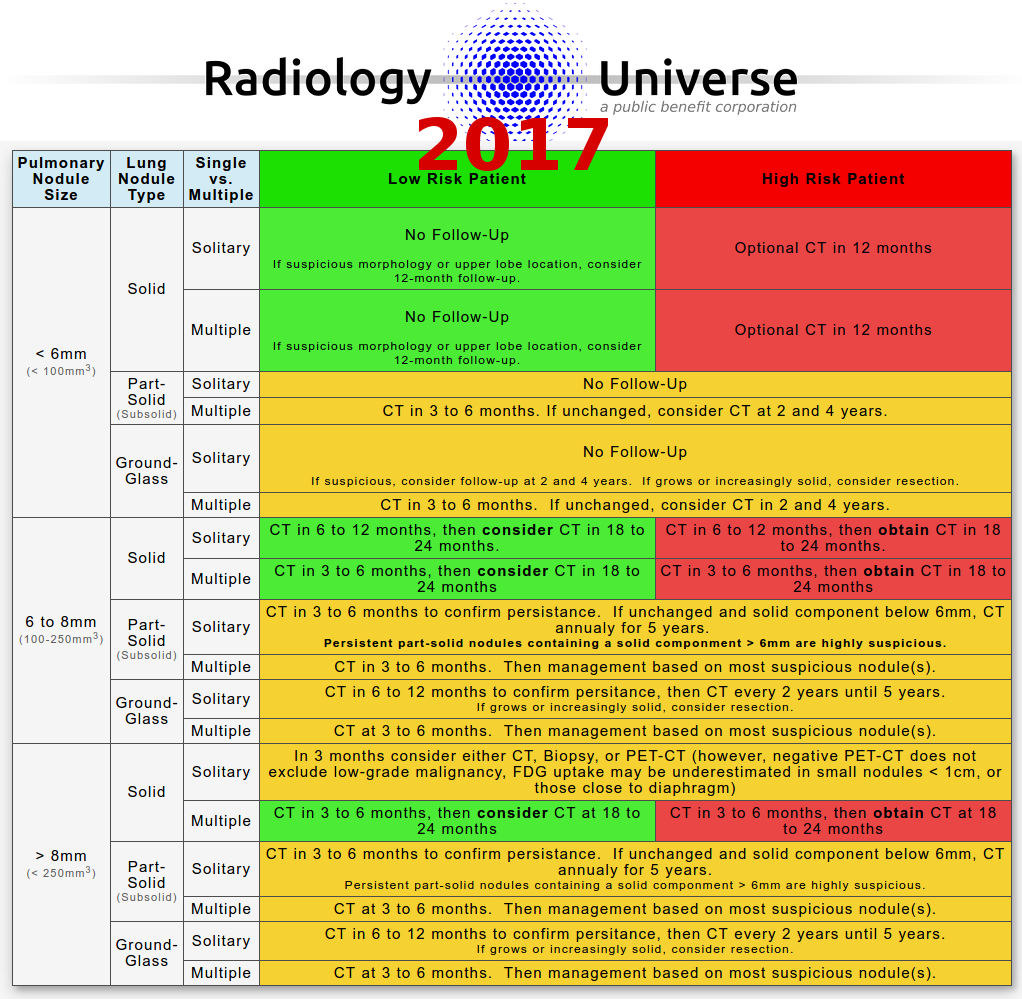
2017 Fleischner Society Pulmonary Nodule Follow-Up Guidelines and Recommendations
for Solid, Subsolid and Ground-Glass Lung Nodules
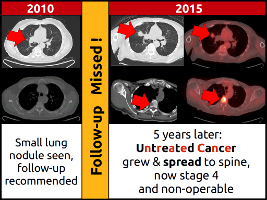
In 51% of cases, physicians fail to obtain the indicated follow-up exams.
| Pulmonary Nodule Size | Lung Nodule Type | Single vs. Multiple | Low Risk Patient | High Risk Patient |
|---|---|---|---|---|
| < 6mm (< 100mm3) |
Solid | Solitary |
No Follow-Up If suspicious morphology or upper lobe
location, consider 12-month follow-up.
|
Optional CT in 12 months |
| Multiple |
No Follow-Up If suspicious morphology or upper lobe
location, consider 12-month follow-up.
|
Optional CT in 12 months | ||
|
Part-Solid (Subsolid) |
Solitary | No Follow-Up | ||
| Multiple | CT in 3 to 6 months. If unchanged, consider CT at 2 and 4 years. | |||
| Ground-Glass | Solitary |
No Follow-Up If suspicious, consider follow-up at 2 and 4
years. If grows or increasingly solid, consider
resection.
|
||
| Multiple | CT in 3 to 6 months. If unchanged, consider CT in 2 and 4 years. | |||
| 6 to 8mm (100-250mm3) |
Solid | Solitary | CT in 6 to 12 months, then consider CT in 18 to 24 months. | CT in 6 to 12 months, then obtain CT in 18 to 24 months. |
| Multiple | CT in 3 to 6 months, then consider CT in 18 to 24 months | CT in 3 to 6 months, then obtain CT in 18 to 24 months | ||
|
Part-Solid (Subsolid) |
Solitary | CT in 3 to 6 months to confirm
persistance. If unchanged and solid component below 6mm, CT annually for 5
years. Persistent part-solid nodules
containing a solid componment > 6mm are highly suspicious. |
||
| Multiple | CT in 3 to 6 months. Then management based on most suspicious nodule(s). | |||
| Ground-Glass | Solitary | CT in 6 to 12 months to confirm persistence, then
CT every 2 years until 5 years. If grows or
increasingly solid, consider resection. |
||
| Multiple | CT at 3 to 6 months. Then management based on most suspicious nodule(s). | |||
| > 8mm (> 250mm3) |
Solid | Solitary | In 3 months consider either CT, Biopsy, or
PET-CT (however, negative PET-CT does not exclude low-grade malignancy, FDG
uptake may be underestimated in small nodules < 1cm, or those close to
diaphragm) |
|
| Multiple | CT in 3 to 6 months, then consider CT at 18 to 24 months | CT in 3 to 6 months, then obtain CT at 18 to 24 months | ||
|
Part-Solid (Subsolid) |
Solitary | CT in 3 to 6
months to confirm persistance. If unchanged and solid component below 6mm,
CT annually for 5 years. Persistent part-solid nodules
containing a solid componment > 6mm are highly suspicious. |
||
| Multiple | CT at 3 to 6 months. Then management based on most suspicious nodule(s). | |||
| Ground-Glass | Solitary | CT in 6 to 12 months to confirm persistence, then
CT every 2 years until 5 years. If grows or
increasingly solid, consider resection. |
||
| Multiple | CT at 3 to 6 months. Then management based on most suspicious nodule(s). | |||
Fleischner Society Recommendations and this table do NOT apply to:
Diameter of lung nodule is the average of the short and long axes, rounded to the whole millimeter.
Lung Cancer Risk Factors:
- Patients who have a known cancer.
- Immunosuppressed patients.
- Lung cancer screening, which has separate criteria.
- Intra-fissural, perifissural, and subpleural pulmonary nodules. Perifissural lung nodules are usually benign, unless suspicious nodule morphology is present (reference).
- Spiculated margins.
- Displacement of the pulmonary fissure.
- Cancer history.
- In these cases, follow-up should be considered.
Diameter of lung nodule is the average of the short and long axes, rounded to the whole millimeter.
Lung Cancer Risk Factors:
- Tobacco use.
- Family history of lung cancer.
- Upper pulmonary lobe location of nodule.
- Presence of emphysema.
- Pulmonary fibrosis.
- Older Age.
- Female gender.
Don't let this happen to Your Patient:
2017 Fleischner Society Lung Nodule Follow-Up Guidelines for Solid, Subsolid and Ground-glass Pulmonary Nodules
{kind=link}
References
- H MacMahon, DP Naidich, JM Goo, KS Lee, ANC Leung, JR Mayo, AC Mehta, Y Ohno, CA Powell, M Prokop, GD Rubin, CM Schaefer-Prokop, WD Travis, PE Van Schil, AA Bankier. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017. Radiology 2017, DOI: http://dx.doi.org/10.1148/radiol.2017161659
- McWilliams, A.; Tammemagi, M. C.; Mayo, J. R.; Roberts, H.; Liu, G.; Soghrati, K.; Yasufuku, K.; Martel, S.; Laberge, F.; Gingras, M.; Atkar-Khattra, S.; Berg, C. D.; Evans, K.; Finley, R.; Yee, J.; English, J.; Nasute, P.; Goffin, J.; Puksa, S.; Stewart, L.; Tsai, S.; Johnston, M. R.; Manos, D.; Nicholas, G.; Goss, G. D.; Seely, J. M.; Amjadi, K.; Tremblay, A.; Burrowes, P.; MacEachern, P.; Bhatia, R.; Tsao, M.-S. & Lam, S. Probability of Cancer in Pulmonary Nodules Detected on First Screening CT New England Journal of Medicine, 2013, 369, 910-919